Introduction
South Korea's healthcare dispute is usually framed as a fight over the number of doctors. The government wants to increase medical school admissions by 2,000 students per year. The medical profession has responded with a large-scale strike involving residents, students, professors, and private practitioners.
That framing is incomplete. Korea does have pressure in emergency medicine, obstetrics, surgery, pediatrics, and some regional markets. The binding constraints, however, sit deeper in the system. They are reimbursement, patient routing, hospital economics, legal risk, and the financing base that supports the insurance system.
This post argues that the current policy response targets headcount while leaving the main incentive structure intact. Korea already delivers strong outcomes on many quality and access metrics. The strain appears where the fee schedule undervalues difficult care, tertiary hospitals absorb excessive demand, and essential specialties carry high workload and legal risk under low reimbursement.
The Current Dispute
In February 2024, the Yoon administration announced a plan to increase annual medical school admissions by 2,000 seats, from 3,058 to slightly above 5,000. The stated goal is to improve staffing in rural areas and essential specialties.
The medical response was immediate. A resident walkout expanded into a much broader labor action. As of August 1, 2024, only 981 of 10,506 residents were working across 211 training hospitals, or 9.3% of the resident workforce (source).
Public support for the increase remains substantial. As of June 2024, 66% of Koreans supported the plan (source). The public case is straightforward. Korea has a low physician-to-population ratio relative to the OECD, very short consultation times, visible strain in emergency and pediatric care, and a rapidly aging population.
Those are real facts. The policy question is whether increasing physician supply addresses the mechanisms producing the observed strain.
The Government's Case
Supporters of the legislation point to six recurring arguments.
First, several essential specialties have persistent recruitment problems. Emergency medicine, obstetrics, general surgery, thoracic surgery, and pediatrics attract fewer trainees than the system needs.
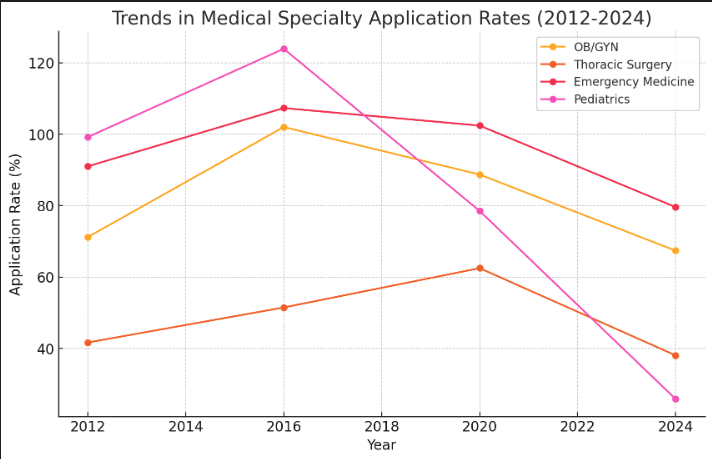
[1] 송수연. (2020, December 5). 갈수록 심해지는 전공의 지원 양극화…"환경 변화 반영". 청년의사 [2] 성서호. (2023, December 7). 내년 소청과 전공의 205명 뽑는데 53명만 손들어…지원율 꼴찌. 연합뉴스. [3] 이창진. (2012, November 29). 인턴들, 복지부 뒤통수…정원 감축후 양극화 심화. 메디칼타임즈.
Second, physician density differs by region. Korea averages roughly 2.3 doctors per 1,000 people, below the OECD average of 3.4. Seoul has about 3.1 per 1,000, while North Gyeongsang has about 1.4 (source).
Third, the aging population will raise utilization. Government materials project a large increase in inpatient and outpatient demand by 2035 as the population over age 65 expands.
Fourth, Korea's doctor-to-population ratio remains low relative to peers such as Germany, France, and the UK.
Fifth, consultation times are very short. Korean primary care visits average about 4.2 minutes, below Japan and far below the US (source, source).
Sixth, physician income appears high in some OECD comparisons. That makes a supply-side explanation intuitive to the public: high pay, visible shortages, and long queues in some specialties are often interpreted as evidence that the country simply needs more doctors.
These facts describe several different bottlenecks.
Thesis
The proposed expansion leaves the main structural drivers of the current crisis in place.
The first driver is reimbursement. Korea sets prices for insured procedures administratively, and every medical institution must participate in the National Health Insurance system. Essential specialties operate inside a fee schedule that has remained low relative to workload, staffing intensity, risk, and inflation.
The second driver is patient flow. Korea has weak gatekeeping and very low barriers to tertiary hospitals. Demand concentrates in large Seoul hospitals while local and secondary institutions lose patients.
The third driver is hospital financing. When covered services are underpriced, hospitals rely on very high patient volume and on non-covered services to remain viable.
The fourth driver is legal exposure. Criminal prosecution for medical negligence is unusually salient in Korea, especially in high-risk specialties.
The fifth driver is the financing base of the system. Korea's healthcare contributions are low relative to other universal systems. A low-contribution system can deliver broad access only if reimbursement remains compressed.
Increasing the number of medical students leaves these mechanisms largely unchanged.
How the System Was Built
South Korea's healthcare system emerged from a private-provider base and then overlaid universal insurance on top of it.
The Medical Insurance Act of 1963 created an early legal framework, but the initial model was voluntary and lacked strong public financing. Access remained poor through the 1960s and early 1970s. A 1972 survey found that only 27% of Seoul residents, 18% of other urban residents, and 2% to 3% of rural residents received medical care. By 1974, 40% of sick people nationwide avoided care, and the rural figure reached 43%.
The government began constructing national health insurance in the mid-1970s. In 1976 it set prices for 413 medical items below prevailing market rates to make the system affordable. Providers objected from the start, and the disagreement over what constituted an adequate fee level became a permanent feature of Korean healthcare politics.
Coverage expanded gradually:
- 1977: firms with 500 or more employees
- 1979: firms with 300 or more employees
- 1981: firms with 100 or more employees
- 1988: rural areas and firms with 5 or more employees
- 1989: urban self-employed households
The critical institutional choice was
당연지정제By 1989, Korea had achieved universal coverage. In 2000, the Kim Dae-jung administration consolidated fragmented insurance societies into a single National Health Insurance Corporation. Coverage expanded further in 2002 when the annual coverage limit was extended to 365 days.
This structure produced a distinctive system: universal insurance, mostly private providers, mandatory participation, and administratively determined prices.
Performance Before the Strike
Any structural analysis should begin with output. Before the current strike, Korea delivered strong performance on many measures of access and clinical quality.
Mortality and Survival
Korea's mortality and survival metrics are strong by developed-country standards.
- Cancer mortality: 159.1 per 100,000 in Korea, 146.2 in the US, 251.6 in the UK, 316.1 in Japan (source, source, source, source)
- Infant mortality: 1.859 per 1,000 live births in Korea, 5.6 in the US, 3.9 in the UK, 1.53 in Japan (source)
- Maternal mortality: 8.4 per 100,000 in Korea, 22.3 in the US, 13.41 in the UK, about 4.5 in Japan (source, source, source)
Korea also has strong five-year cancer survival.

- Korea: 72.1%
- US: 69%
- UK: 55.7%
- Japan: 66.2%
Readmissions and Preventable Mortality
Korea's 30-day readmission rate is 5.9%, compared with 14.5% in the US and 11.6% in the UK. Japan performs at 3.4% (source, source, source, source)
Preventable mortality is also low. Korea ranks eighth in the OECD at 99 deaths per 100,000. That places it ahead of France, Canada, Germany, the UK, and the US.
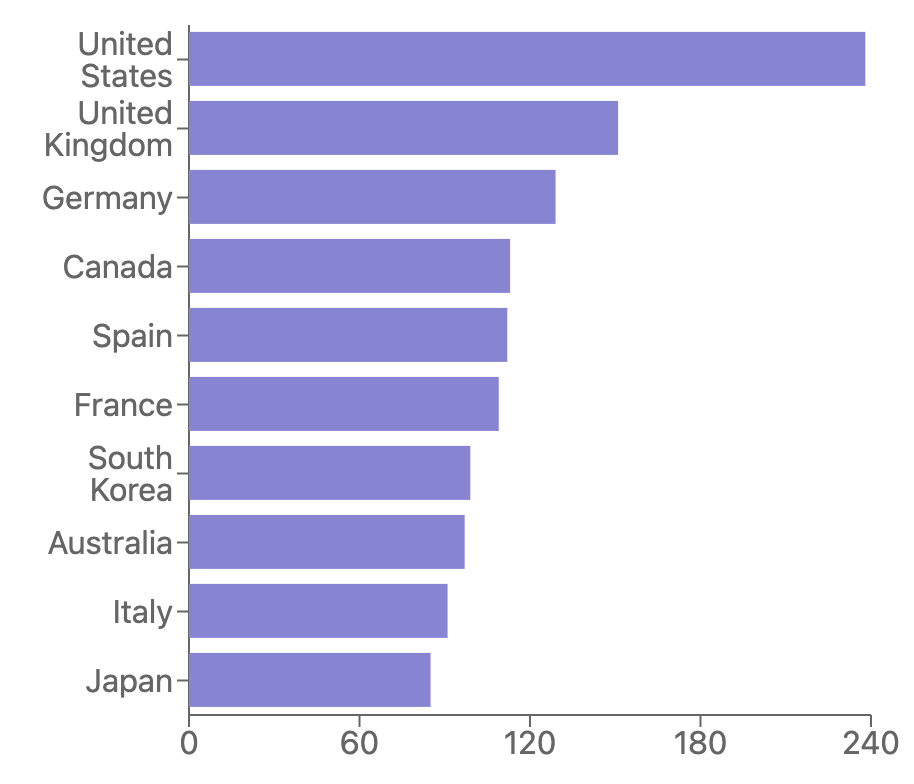
Mortality rates from preventable causes in OECD countries in 2021.
Access
Korea's access metrics are unusually strong.
Patients can see specialists directly without a formal referral chain. About 51.3% of patients walk into tertiary hospitals and are examined immediately (source). In the "big 5" hospitals, 75% of patients see their specialist of choice within one month.
Regional physician distribution also looks more balanced in OECD regional data than the popular narrative suggests. Korea records 2.77 physicians per 1,000 in urban areas and 2.0 in rural areas. Only Switzerland and Norway show smaller urban-rural gaps in that dataset.
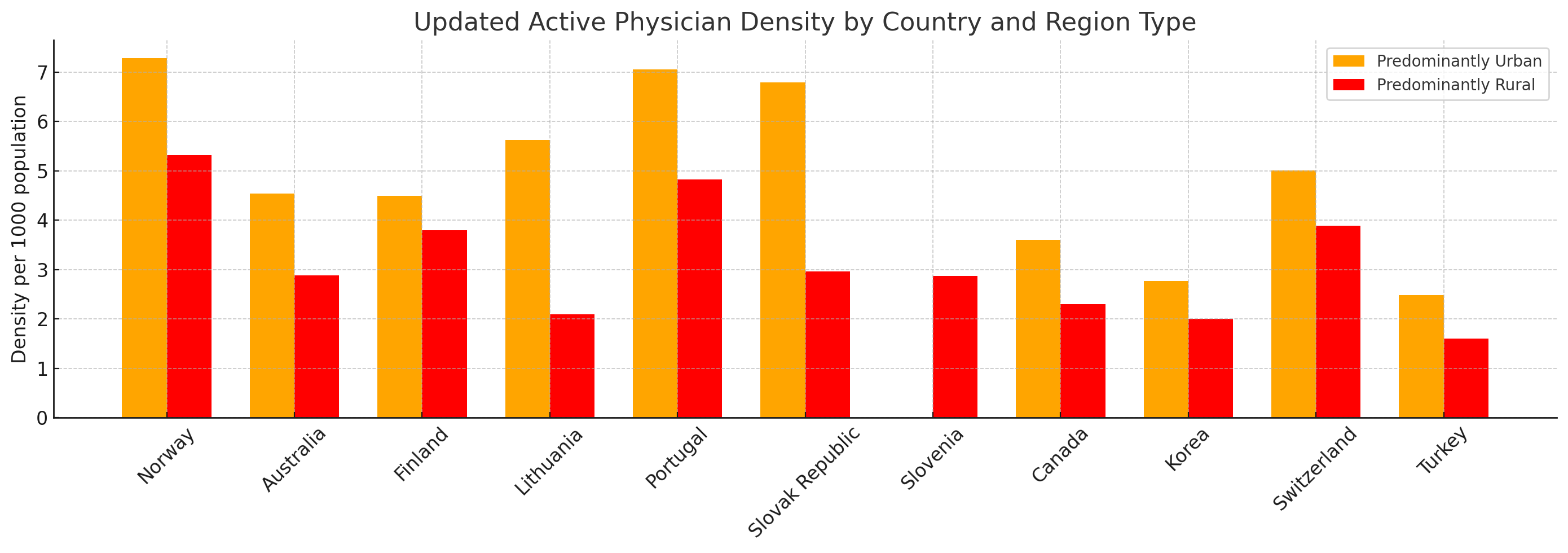
OECD Regional social and environmental indicators, 2021.
The system therefore combines high access with strong output. The current problem is sustainability.
The Price System
The central feature of Korean healthcare economics is the fee schedule.
A fee schedule is the list of amounts that insurance pays providers for covered services. In Korea, those prices are set administratively through the National Health Insurance system. The prices are uniform across participating providers, and patients are entitled to covered care from every institution because participation is mandatory.
For several classes of treatment, especially DRG-covered procedures, the prices are explicit and fixed. Those prices determine hospital revenue for labor, equipment, facilities, nursing, and overhead.
This creates a basic tension. Low prices expand access and keep household spending low. Low prices also compress provider margins and make difficult, labor-intensive specialties hard to sustain.
To compare prices internationally, I normalize Korean fee-schedule amounts using 2022 GDP per capita PPP. Korea was at $53,759.58 and the US at $77,191.87, giving a ratio of about 1:1.43 (source).
Concrete Price Examples
Emergency visit
- US Medicare fee schedule for CPT
: about $130.6199284 - US cash price: about $699
- Korea emergency specialist visit fee: $29.96
- PPP-adjusted Korea fee: $42.84
- UK tariff: about $99.09
V2200,2024-01-01,응2가,응급진료 전문의 진찰료-권역응급의료센터,,1,0,0,41540 VB11Z Emergency Medicine, No Investigation with No Significant Treatment 91 euros
Chest CT
- US fee schedule for CPT
: about $177.0871260 - US average total payment: about $175 to $228
- US cash price: about $2,000
- Korea fee schedule: $74.95
- PPP-adjusted Korea fee: $107.17
- Korea cash prices observed: about $141.75 to $189.72
- UK tariff: about $80.57
HA464007,2024-01-01,다245라(2),일반전산화단층영상진단-흉부-조영제를사용하는경우,Chest CT-With Contrast Material,1,0,103930 RD20A Computerised Tomography Scan of One Area, without Contrast, 19 years and over 74
Stroke care
For acute ischemic stroke:
- Korea tPA drug price: $415.76
- Korea tPA administration fee: $138.10
- PPP-adjusted Korea totals: $594.53 for the drug and $197.48 for administration
- US tPA drug price: about $4,642
- US administration estimate: about $10,098
- UK tPA drug price: about $326
- UK administration estimate: about £1,316
Mechanical thrombectomy shows the same pattern:
- Korea fee schedule: $842.91
- US average total payment: above $11,500
- UK tariff estimate: about $12,793.75
경피적혈전제거술-기계적혈전제거술[카테터법]-두개강내 혈관,Percutaneous Thrombus Removal-Mechanical thrombectomy(Intracranial vessel),1160620
Cataract surgery
- Korea fee schedule: $327.80
- PPP-adjusted Korea fee: $468.75
- Korea tertiary DRG amount: $999.84
- US fee schedule: $602.37
- US average total payment: $2,220.35
- UK tariff: $834.18
백내장및수정체수술-수정체낭외또는낭내적출술,Surgery for Cataract Or Lens-Extracapsular Or Intracapsular Extraction,2,9,453980 BZ32B Intermediate, Cataract or Lens Procedures, with CC Score 0-1 - 766
Cesarean section
- Korea surgeon fee: $345.52
- PPP-adjusted Korea surgeon fee: about $494
- Korea tertiary DRG amount: $2,487.50
- PPP-adjusted Korea DRG amount: about $3,557
- US fee schedule for CPT
: about $987.7759514 - US average total payment: $18,570
- UK tariff: about $4,144.58
제왕절개만출술(1태아임신의경우)-초회(초산),Cesarean Section Delivery-First Fetus-Initial-Primiparous,475750 NZ50C Planned Caesarean Section with CC Score 0-1: payment level 3
The pattern is consistent across routine, diagnostic, and highly specialized care. Korea purchases medical labor and infrastructure very cheaply.
What Low Prices Do to the System
Low reimbursement affects behavior across the entire delivery chain.
High patient volume
When visits are cheap, volume becomes the primary way to sustain revenue.
Koreans average 15.7 doctor visits per year, compared with 11.1 in Japan, 6.0 across the OECD, and 3.4 in the US. Extreme cases are also visible in the administrative data. One patient reportedly visited 24 hospitals 2,050 times in 2021 (source).
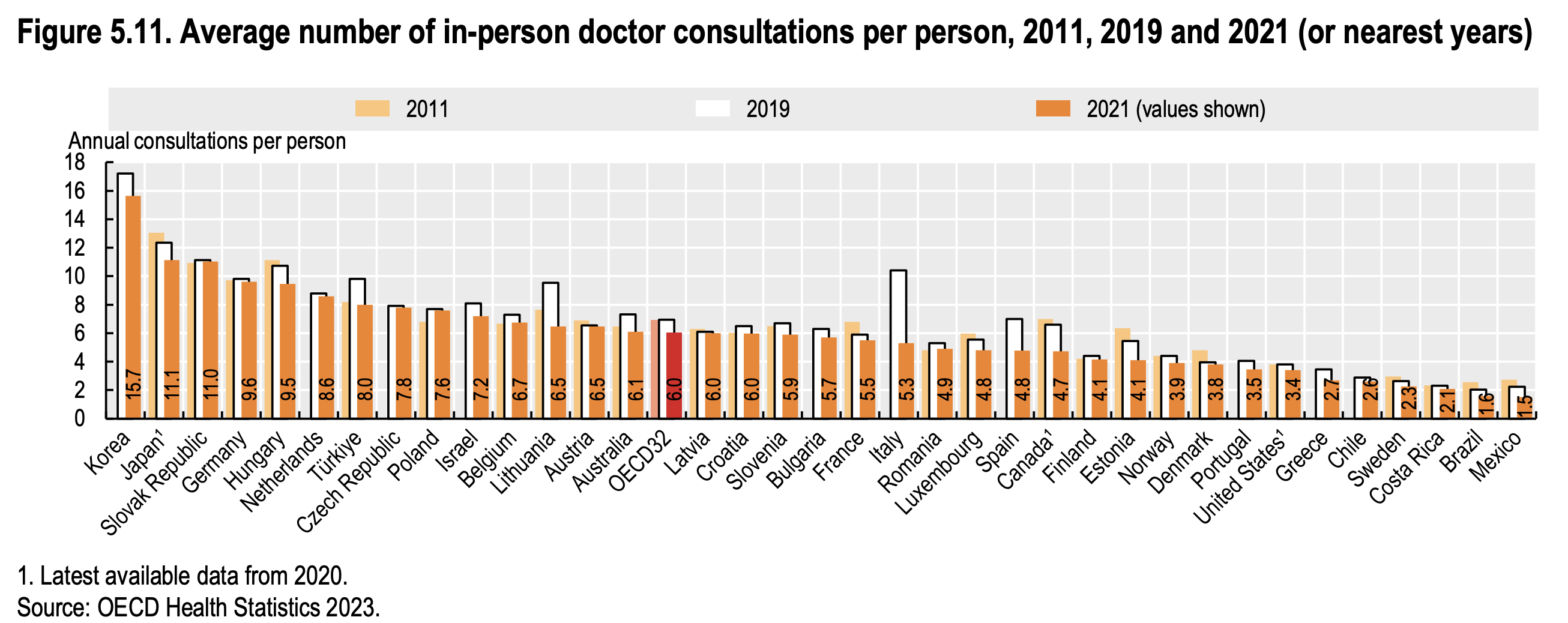
[OECD (2023). "Consultations with doctors". In Health at a Glance 2023: OECD Indicators. Paris: OECD Publishing.](https://www.oecd-ilibrary.org/docserver/3a4927d8-en.pdf?expires=1721352973&id=id&accname=guest&checksum=B818F42A56EF3645A5AE443664D7E3E2#:~:text=In 2021%2C the average number,reporting between 4 and 10)
A 2020 survey of 6,507 doctors shows the operational consequence (source):
- Average daily patient load: 37.8
- Primary care clinics: 43.0
- Most visits: 6 to 10 minutes
- Follow-up visits under 5 minutes: 65.5%
Short consultations follow directly from the reimbursement model and the volume it induces.
Demand concentration in tertiary hospitals
Korea formally built a tiered delivery system in 1989, with primary, secondary, and tertiary levels. In practice, access to tertiary care remains unusually open.
Earlier regional referral structures were weakened over time. Patients can travel to Seoul and large university hospitals with limited friction. Financial and administrative differences between hospital tiers are also small relative to the perceived quality differences.
The result is demand concentration. Tertiary hospitals absorb a growing share of spending while local clinics and regional hospitals lose patients.
- In 2018, large hospitals increased expenses by 19.8% to 26.6 trillion won, and their market share rose from 32% to 34.3% (source)
- In 2023, tertiary hospitals' share of medical costs reached 19.8%, up from 16.8% in 2022 (source)
This matters for the rural debate. A regional shortage can be caused by weak local demand, weak referral structure, and concentrated patient preferences while physician density remains within a relatively narrow range.
Reliance on non-covered items
Korea's insured price schedule is too compressed to support every institution and specialty equally well. Hospitals and clinics therefore rely on non-covered items.
Non-covered services include vision correction, some dental work, manual therapy, many certificates, some imaging, and a range of elective or semi-elective services. Providers can price these directly.
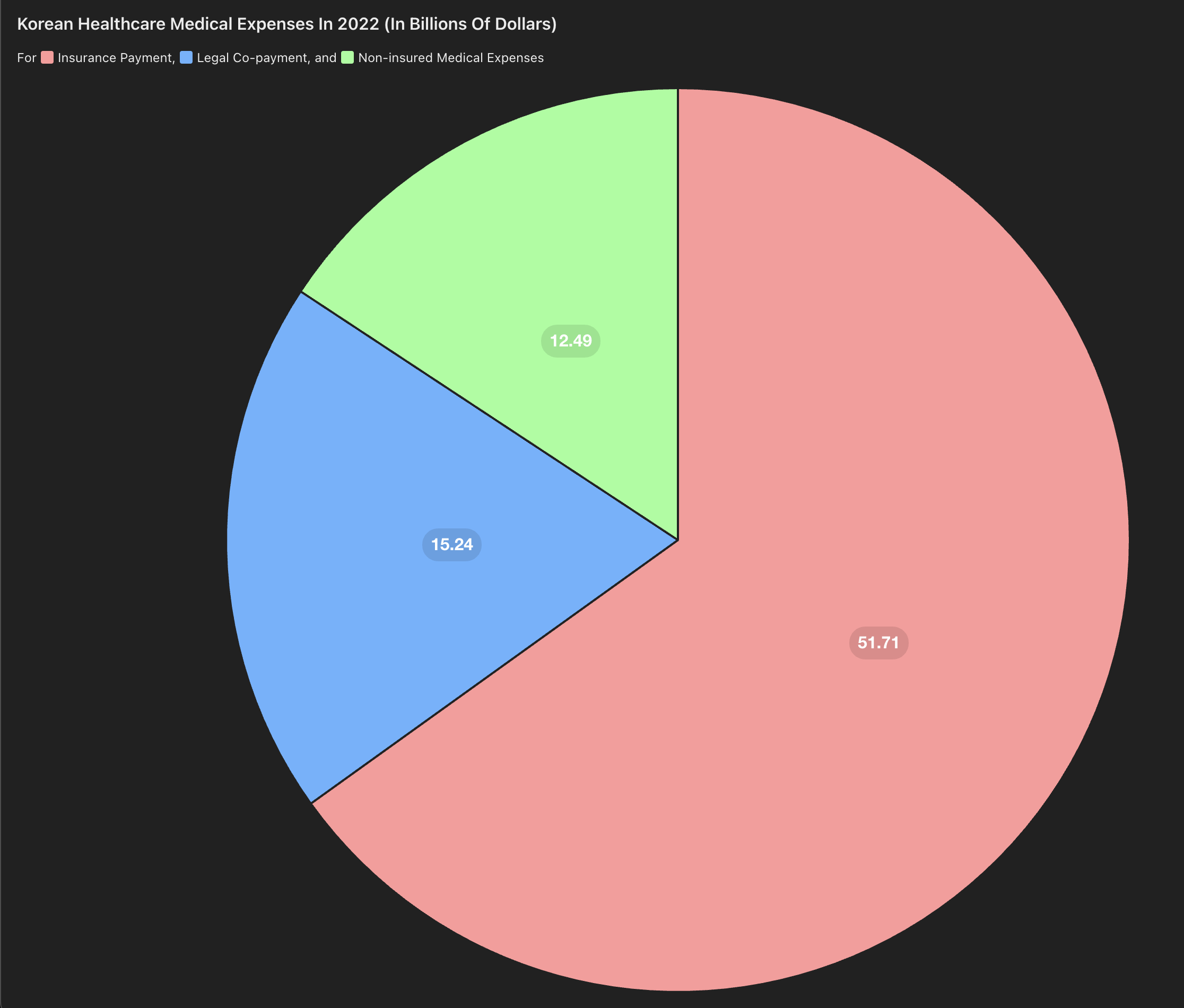
This spending is large:
- Total medical spending in 2022: 111.1 trillion won
- Government/NHI share: 71.6 trillion won, or 64.4%
- Legal out-of-pocket share: 22.1 trillion won, or 19%
- Non-covered items: 17.3 trillion won, or 15.5%
이정환. (2023, January 10). 작년 보장률 64.5%...0.8%p 하락 "비급여 관리". 데일리팜
The dependence is uneven across the system. Local clinics can orient themselves toward profitable outpatient markets. Tertiary hospitals must also maintain emergency departments, ICUs, training programs, and difficult specialties that consume staff and capital.
That distribution changes physician behavior. When difficult covered work is persistently underpriced, physicians migrate toward fields with better pricing power.
Hospital Economics
The hospital balance sheet reflects the same compression.
Data from major hospitals between 2017 and 2019 show thin margins:
| Hospital Name | Total Revenue (in $ million) | Total Expenses (in $ million) | Profit Before Tax (in $ million) | Reserve for Inherent Business Purpose (in $ million) | Reversal of Reserve (in $ million) | Net Profit (in $ million) |
|---|---|---|---|---|---|---|
| Samsung Seoul Hospital | 3,133 | 3,210 | -77.2 | 0 | 4 | -73.3 |
| Severance Hospital | 3,261 | 3,026 | 222.7 | 269.8 | 0 | -47.1 |
| Asan Medical Center | 4,035 | 3,894 | 141.2 | 118.4 | 0 | 22.7 |
| Bundang Seoul National University Hospital | 1,746 | 1,674 | 71.3 | 89.4 | 36.3 | 16.3 |
| Seoul National University Hospital | 2,645 | 2,618 | 26.5 | 40.3 | 15.1 | -1.2 |
Source: Medical Times
Across 3,200 hospitals in a 2015 survey, the average margin was 1.9%. Tertiary hospitals were slightly negative on average (source).
These margins show a system operating close to minimum viable economics.
Reserve funds also need to be interpreted correctly.
고유목적사업준비금From a system perspective, the more important fact is that Korean hospitals achieve service volumes and access levels that would normally require higher reimbursement.

이지현. (2020, October 6). 외래수익으로 확연히 드러난 빅5 쏠림...."정부 정책 패착". 메디칼타임즈.
US hospitals often receive roughly 60% of revenue from inpatients and 40% from outpatients. Korean hospitals can arrive at similar revenue structure only by processing far more outpatient volume (source).
Essential Specialties and Legal Risk
Shortages in emergency medicine, obstetrics, surgery, and pediatrics reflect both economics and liability.
Korea's criminal treatment of medical negligence is unusually forceful. The reported annual charge rate for occupational negligence death is about 0.5% of Korean doctors, versus about 0.01% in Japan (source). Trial outcomes also show a higher share of convictions in Korea than in Japan.
- Korea: 354 trials over 11 years, 239 guilty
- Japan: 202 trials over 18 years, 32 guilty
The UK and US frameworks are narrower. Criminal prosecution is generally reserved for extreme conduct, gross negligence, or intentional wrongdoing, while most malpractice disputes remain civil (source, source).
This changes specialty choice. High-risk acute care fields already carry difficult hours, staffing pressure, and emotionally costly outcomes. Adding significant criminal exposure reduces the supply of physicians willing to remain in those specialties.
Why Rural Access Remains Difficult
Rural access is usually described as a simple staffing gap. The data suggests a more complicated mechanism.
Korea's urban-rural physician gap is present, but smaller than many observers assume in OECD regional data. At the same time, patients continue to travel toward large hospitals and Seoul-based institutions. That indicates a demand-allocation problem as well as a supply problem.
Local hospitals require patients, referrals, revenue, staff, and capital to remain credible. When patients can easily bypass them, local institutions lose the case volume needed to sustain quality. That lowers demand further and weakens the local hospital base.
A physician in Miryang described a five-year decline in patient volume, including an 8% drop from 2022 to 2023 and a 20% drop in patients in early 2024 (source). A policy focused only on physician headcount leaves this feedback loop intact.
The Financing Constraint
Korea runs a very low-contribution universal health system.
This is visible from both top-down and bottom-up measures. Total health expenditure is low relative to peers. Household and employer contributions are also low relative to several other universal systems.
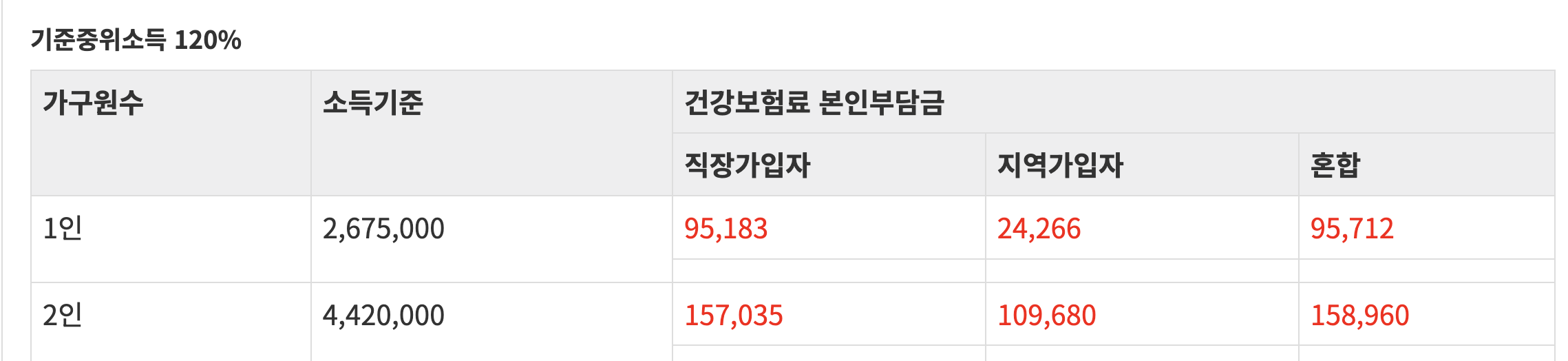
For a household at roughly 120% of median income, Korea's National Health Insurance premium is about 7.09% of payroll, split between employee and employer. That leaves the employee paying roughly 3.5% directly and the employer paying roughly 3.5%.
Comparable burdens are higher elsewhere:
- UK: roughly 20% combined employee and employer National Insurance at median earnings (source)
- Japan: about 9.98% in Tokyo, split between employee and employer (source)
- Norway: 21.9% combined contributions (source, source)
- Canada: no dedicated payroll tax in the same form, but estimates of the implicit cost still place the burden well above Korea in many cases (source)
The financing implication is direct. A low-contribution system must either spend less overall, ration access more aggressively, or compress provider reimbursement. Korea chose low household burden and broad access, which leaves compressed reimbursement doing much of the balancing work.
Talent Allocation
Korea's healthcare system has benefited from a separate national characteristic: medicine captures a large share of top academic talent.
Medical school admissions remain one of the most competitive paths in the country. In public university admissions, repeat test-takers make up a very large share of those pursuing medicine. Medicine and dentistry dominate university-major prestige rankings, often above strong engineering programs.

This matters because a low-price healthcare system is easier to sustain when a large fraction of high-performing students continue to enter medicine despite the compressed reimbursement environment. Korea has historically benefited from that equilibrium.
The broader economic issue is that Korea offers fewer alternative prestige and compensation paths than countries with deeper venture, finance, and research ecosystems. Medicine therefore functions as both a profession and a national talent sink.
That has helped preserve quality. It also means the system depends on a career pipeline that may weaken if relative returns fall further.
Policy Implications
A physician supply increase can change long-run capacity. The current allocation problem requires additional reforms.
The more direct levers are:
- Raise consultation fees so physician time is priced less aggressively at the low end.
- Increase reimbursement substantially for difficult covered work in emergency medicine, obstetrics, surgery, pediatrics, and other avoided specialties.
- Reduce criminal exposure for ordinary medical negligence and align liability more closely with international practice.
- Rebuild a referral-based primary care structure so tertiary hospitals focus on complex cases.
- Create stronger financial and administrative incentives for patients to use local and secondary hospitals when clinically appropriate.
- Increase the funding base of the system if the public wants to preserve both universal access and high-quality covered care.
These are financing and incentive reforms. Headcount policy works best after those mechanisms are addressed, because specialty choice and hospital viability respond to the underlying price and risk structure.
Expected Direction Under Current Policy
If the current approach remains focused on physician headcount alone, several outcomes are likely.
First, conflict between the state and the profession will continue. Second, tertiary hospitals will remain overloaded. Third, essential specialties will continue to struggle with recruitment and retention. Fourth, hospitals will keep relying on volume and non-covered items. Fifth, regional institutions will remain weak. Sixth, public frustration will rise as visible shortages persist despite an increase in training slots.
The broader point is that Korea's healthcare system is a high-performing system operating under a strained financing and incentive design. The present dispute has made that design visible.
Sources
- US fee schedule: CMS Physician Fee Schedules
- US average total payment amount: Google Sheet, Medicare procedure lookup
- US cash price data: Turquoise Health
- UK tariff workbook: NHS Payment Scheme Annex A 2024-25
- Korea fee schedule: Fee schedule spreadsheet, 2019 급여기준 및 심의사례집
- Korea DRG amounts: HIRA DRG amount list, 2024 DRG cost notice